Updated feb 2019
Bottom line:
Consanguinity is defined as a union between two individuals who are related as second cousins or closer. The chance for adverse outcome in the offspring of a consanguineous union is an estimate based on family history, degree of consanguinity and background population risk. In general, studies have shown that, when there is no known genetic diagnosis in the family, first cousin unions are at a 1.7-2.8% additional risk above the general population risk of 2-3% to have offspring with a congenital anomaly. The risk for a more closely related union is higher and for a more distantly related union is lower. The best tool for counselling a couple about consanguinity is a detailed family history. Genetic testing based on ethnicity, and standard prenatal screening should be offered as for non-related couples. Referral for genetic consultation can be considered if appropriate based on family history and/or screening results.
What is Consanguinity?
One billion of the current global population lives in communities with a preference for consanguineous union. Consanguinity is defined as a union between two individuals who are related as second cousins or closer.2
In North African, Middle and West Asian, and South Indian populations (and immigrants from these communities) about 20-50% of all unions are consanguineous and first cousin unions account for about 1/3 of all marriages. See Figure 1 for global distribution of consanguinity rates. Reasons for preferring a consanguineous union can include cultural continuity, family solidarity, or reduction of uncertainty associated with health and financial issues. Primary healthcare providers are likely to see couples in consanguineous unions from these communities who are seeking preconception/prenatal counselling.2
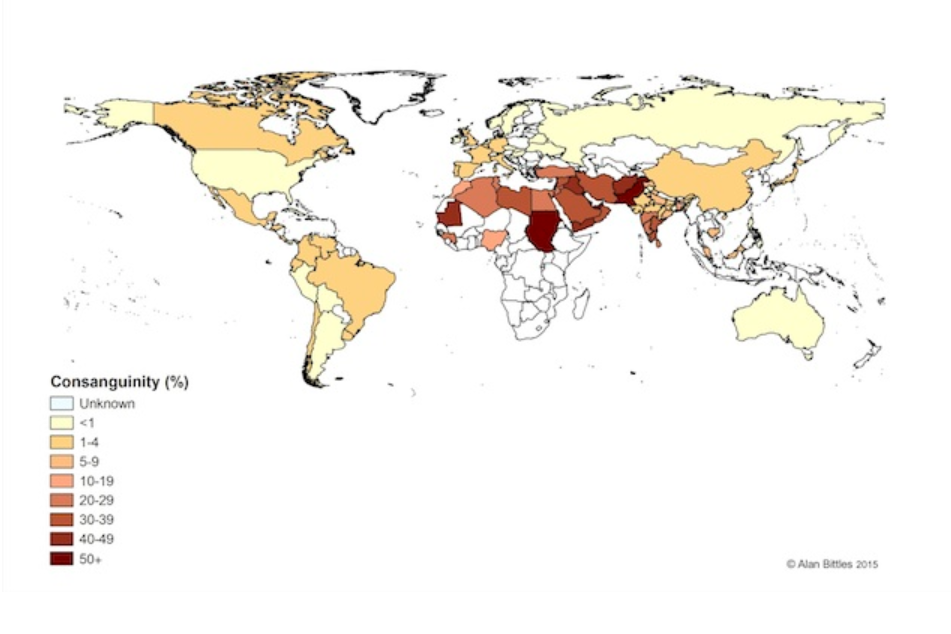
Figure 1. Global distribution of consanguinity rates.3
What do I need to know about the genetics of Consanguinity?
Inbreeding and consanguinity are terms often used interchangeably, although inbreeding is a derogatory term when applied to humans.1 However, this term persists in population genetics and has some utility. The coefficient of inbreeding (F) provides a numerical risk estimate for the degree of inbreeding of an individual. F values are higher for unions that are more closely related (see Figure 2).1 F can be thought of as the proportion of genes in the offspring of a consanguineous union where the copy inherited from each parent is identical i.e. the proportion of loci at which an individual is homozygous from the same ancestral source.1
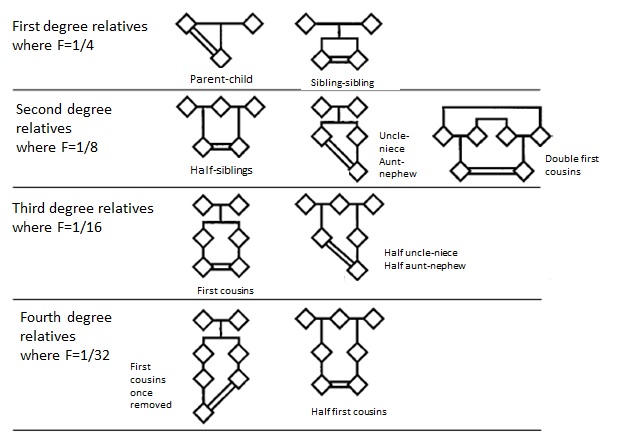
Figure 2. Examples of consanguineous unions.1
See What does consanguinity mean for my patients? for information on risks for offspring of a consanguineous union.
Who should be offered genetic testing and/or referral?
The first step and best tool for counselling a couple with consanguinity involves taking a detailed family history. A four-generation pedigree is ideal for documentation and discussion with the patient.1,2 Patients can confuse familial relationships such as second cousins with first cousins once removed, and, in some cultures, non-biological relatives may be referred to as “uncle” or “aunt” and can be confused with blood relatives.1 Download the GEC-KO Family History Tool to assist you in eliciting and drawing the family history.
When taking the family history, be specific in your questions and note:
- Offspring, siblings, parents, grandparents, aunts, uncles, nieces, nephews, and first cousins of your patient, as appropriate
- Ethnicity of all grandparents
- Congenital anomalies or birth defects
- Early hearing and/or vision impairment
- Failure to thrive
- Intellectual disability, learning disability, developmental delay or regression
- Inherited blood disorders (e.g. thalassemia)
- Unexplained neonatal or infant death
- Seizure disorder
- Undiagnosed severe conditions
Genetic testing based on ethnicity and standard prenatal screening should be offered as for non-related couples. Referral for genetic consultation can be considered if appropriate based on abnormal screening results of family/personal history such as1,2:
Family history positive for congenital anomalies
Both members of the couple are carriers of the same genetic condition
Both members of the couple are carriers of a hemoglobinopathy. Even if each parent is a carrier of a different type of beta hemoglobinopathy (e.g. one parent is a carrier for sickle cell disease and the other parent is a carrier for beta thalassemia), the possible genetic combination in their children could result in an inherited blood disorder.
What does consanguinity mean for my patient?
The chance for adverse outcome in the offspring of a consanguineous union is not an absolute number but rather an estimate based on family history, degree of consanguinity and background population risk.1
In general, studies have shown that, when there is no known genetic diagnosis in the family, first cousin unions are at a 1.7-2.8% additional risk above the general population risk of 2-3% to have offspring with a congenital anomaly, for example a congenital heart defect, which is the most common multifactorial congenital anomaly.1,2 The risk for a more closely related union is higher and for a more distantly related union is lower. There is an increased risk of autosomal recessive conditions in the offspring of consanguineous unions. The closer the biological relationship between the couple, the higher the chance their offspring will inherit identical copies of one or more detrimental recessive genes from each parent.2 It is unclear whether consanguinity increases the risk for later onset complex disorders such as diabetes or cardiovascular disorders.1,2
There is a 3.5-4.4% increased risk (above population risk) for children of consanguineous unions to die before the age of 10 years.1,2
Ethinicity-based screening
Certain genetic disorders are more common in populations likely to prefer consanguineous unions (e.g. hemoglobinopathies). Screening for carrier state is recommended by the Society of Obstetricians and Gynaecologists of Canada (SOGC) Genetics Committee and the Canadian College of Medical Geneticists (CCMG) Clinical Practice Committee for individuals belonging to population groups known to have an increased risk for carrying certain genetic disorders.4 Preconception counselling and testing is recommended in order to arrange for prenatal testing if appropriate. See the GEC-KO Point of Care Tool for more on reproductive genetic carrier screening in Canada.
How do I order genetic testing?
The process of ordering genetic testing depends on the specific carrier screening that is required. Please contact your local genetics centre for further information regarding how to order reproductive genetic carrier screening in your province. In Ontario, Ashkenazi Jewish reproductive screening is performed on a blood sample that is sent to the laboratory at The Hospital for Sick Children for analysis. To order this screening, please attach the Hospital for Sick Children Carrier Screening: Tay Sachs Enzyme Testing and Ashkenazi Jewish Molecular panel requisition, along with the regular Ministry of Health blood requisition, to the blood sample drawn from your patient(s). If you require a different form of reproductive screening for your patient, please contact your local genetics centre.
Where do I refer my patient?
Click the link to contact your local genetics centre
Note that genetics clinics vary with regard to the referrals they choose to accept. You may want to contact your local centre for more information.
Include all relevant information on your referral (e.g. family history, genetic test results, and investigations like hemoglobin electrophoresis) to prevent unnecessary delays due to further clarification needed before an appointment can be booked.
Resources for health professionals
[1] Hamamy, H. Consanguineous marriages: Preconception consultation in primary health care settings. J Community Genet 2012; 3:185-192
[2] Bittles AH and Black ML (2013) Global Patterns & Tables of Consanguinity. http://consang.net
[3] Bennett RL, Motulsky AG, Bittles A, et al. Genetic counselling and screening of consanguineous couples and their offspring: recommendations of the National Society of Genetic Counselors. J Genet Couns 2002; 11(2):97-119
[4] Wilson RD, De Bie I, Armour CM, et al. Joint SOGC-CCMG Opinion for Reproductive Genetic Carrier Screening: An Update for All Canadian Providers of Maternity and Reproductive Healthcare in the Era of Direct-to-Consumer Testing. J Obstet Gynaecol Can 2016; 38(8):742-762.e3
Resources for patients and the public
Links to provincial newborn and prenatal screening programs can be found on the GEC-KO website www.geneticseducation.ca in the Public Resources section as can contact information for your local genetics centre.
Canadian Paediatric Society position statement on Universal Newborn Hearing Screening
Consanguinity/Endogamy Resource. Worldwide statistics on marriages between first cousins, uncles and nieces, and other consanguineous relationships. http://consang.net
Authors: S Morrison MS CGC, JC Carroll MD CCFP and JE Allanson MD FRCPC
Updated by the GECKO team: S Yusuf MS CGC, JC Carroll MD CCFP, JE Allanson MD FRCPC FCCMG
Disclaimer:
· GECKO is an independent not-for-profit program that does not accept support from commercial or non-academic entities.
· GECKO aims to aid the practicing non-genetics clinician by providing informed resources regarding genetic/genomic conditions, services and technologies that have been developed in a rigorous and evidence-based manner with periodic updating. The content on the GECKO site is for educational purposes only. No resource should be used as a substitute for clinical judgement. GECKO assumes no responsibility or liability resulting from the use of information contained herein.
· All clinicians using this site are encouraged to consult local genetics clinics, medical geneticists, or specialists for clarification of questions that arise relating to specific patient problems.
· All patients should seek the advice of their own physician or other qualified clinician regarding any medical questions or conditions.
· External links are selected and reviewed at the time a page is published. However, GECKO is not responsible for the content of external websites. The inclusion of a link to an external website from GECKO should not be understood to be an endorsement of that website or the site’s owners (or their products/services).
· We strive to provide accurate, timely, unbiased, and up-to-date information on this site, and make every attempt to ensure the integrity of the site. However, it is possible that the information contained here may contain inaccuracies or errors for which neither GECKO nor its funding agencies assume responsibility.

