
Download the PDF here. Download the triage and surveillance point of care tool.
Bottom line: Hereditary Hemochromatosis (HH) is a common inherited iron overload disorder. Affected individuals are predisposed to absorb excess iron from their diet due to improper regulation of iron homeostasis. Over time excess iron can be deposited in organs leading to dysfunction. The most common type is caused by pathogenic variants in the HFE gene. The C282Y variant in this gene is associated with highest risk for iron overload. HFE-related HH is an autosomal recessive condition where one must inherit two pathogenic variants (one from each parent) to be at risk for iron overload. Most individuals with this predisposition do not develop clinical disease. While HH does have the potential to cause morbidity and mortality, with early identification of at-risk individuals, appropriate surveillance of iron indices, and treatment (phlebotomy) when necessary, many complications can be avoided.
Genetic testing should be considered for adults with:
- Biochemical evidence of iron overload [>45% fasting transferrin saturation and elevated serum ferritin (>300 ug/L in men and post-menopausal women, >200 ug/L in pre-menopausal women)]
- Unexplained chronic liver disease and increased transferrin saturation
- A first-degree relative where genetic testing identified C282Y homozygosity (2 copies of the C282Y pathogenic variant)
- Symptoms of iron overload and a first-degree relative where genetic testing identified at least one copy of the C282Y pathogenic variant
- A family history confirmed or suggestive of hereditary hemochromatosis
Updated July 2023
WHAT IS HEREDITARY HEMOCHROMATOSIS?
Hereditary Hemochromatosis is an inherited predisposition to absorb excess iron from the diet. Body iron stores are regulated only at the level of absorption as there is no process for elimination of excess. Over time excessive iron absorption can lead to subsequent storage in various organs (i.e. liver, pancreas, heart, joints) eventually leading to cellular injury. If untreated, eventually this can cause irreversible tissue/organ damage and shorten life expectancy.
What are the genetics of hereditary hemochromatosis?
There are different types of hereditary hemochromatosis (HH) as defined by the deficient protein/gene involved in iron homeostasis. The most common cause is due to pathogenic variants in the HFE gene (known as Type 1 or HFE-related). HH is inherited in an autosomal recessive manner, so an individual must inherit a pathogenic variant from each parent (one pathogenic variant in each HFE gene) in order to be at risk for iron overload.
Standard genetic testing for HFE-related HH is targeted. This means that molecular genetic laboratories look only for the presence of specific pathogenic variants in the HFE gene. The two most common pathogenic variants in HFE are named C282Y and H63D. These variants account for over 90% of HFE-related HH. The C282Y variant is the most common and in the homozygous state is most likely to result in iron overload (i.e. C282Y/C282Y genotype). Other genotypes are possible i.e. C282Y/S65C, H63D/H63D, S65D/S65C, but are not considered clinically significant i.e. not likely to cause increased risk for iron overload. Table 1 shows the associated risk of iron overload with an associated genotype.
Genetic testing for non-HFE related hereditary hemochromatosis is possible but not recommended.
How common is HFE-related hereditary hemochromatosis?
About 1 in 3 individuals of northern European ancestry (highest for Irish and Scandinavian ancestry) are carriers (heterozygotes) of the C282Y or H63D HFE pathogenic variant.
About 1 in 150 individuals have two copies of (are homozygous for) the C282Y HFE gene pathogenic variant (genotype C282Y/C282Y). Of individuals with clinical manifestations of HH, about 80% can be attributed to C282Y/C282Y
Table 1. Risk of iron overload associated with genotype.
|
Genotype |
Associated risk of iron overload |
|
C282Y/C282Y |
|
|
C282Y/H63D |
|
WHAT ARE THE SYMPTOMS OF HEREDITARY HEMOCHROMATOSIS?
Typically, symptoms of HFE-related hereditary hemochromatosis (HH) present in men aged 40 to 60 and in post-menopausal women; however, age of onset is variable.
Diagnosis of HH is difficult as symptoms are non-specific and broad. Weakness, lethargy, and joint pain are the most common symptoms in early clinical presentation. Awareness of HH is fundamental to provoking clinical suspicion. Some individuals can have hepatic iron overload even in the absence of clinical presentation. Additional clinical features of HH are shown in Figure 1.
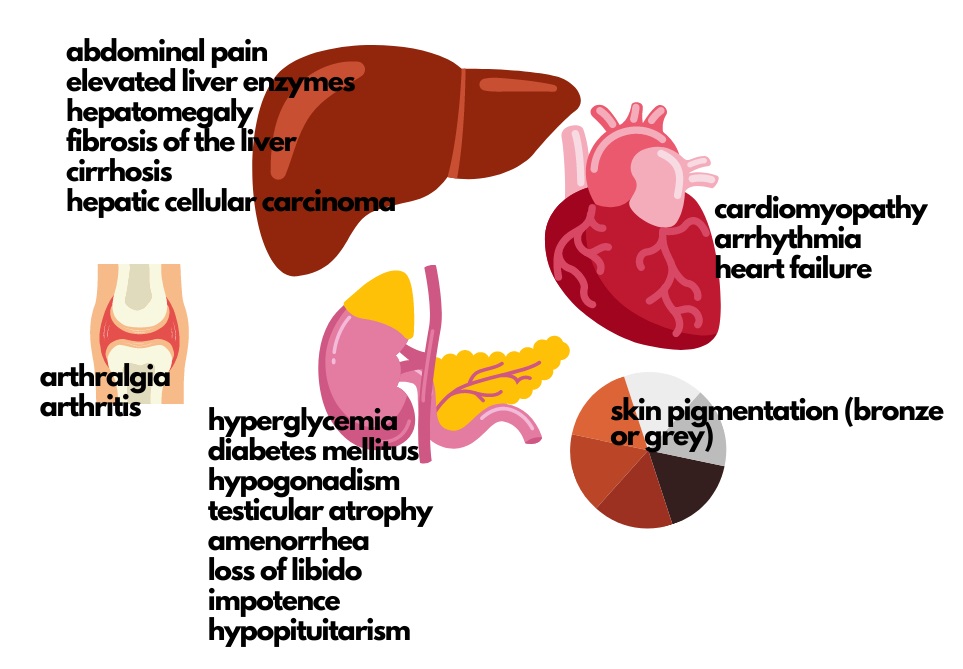
Figure 1. Clinical presentation of hereditary hemochromatosis. (Adapted from Kowdley et al. 2019)
While any of these health concerns can be caused by HFE-related HH, the presence of two or more should greatly increase suspicion that the condition is present.
Iron overload due to pathogenic variants in the HFE gene does not occur in childhood as HH is an adult-onset predisposition.
With early identification of at-risk individuals, appropriate surveillance of iron indices, and treatment when necessary, many complications can be avoided.
WHAT IS THE TREATMENT FOR HEREDITARY HEMOCHROMATOSIS?
Phlebotomy is the first-line treatment for hereditary hemochromatosis (HH).
Treatment usually occurs weekly and is monitored by a specialist (e.g. gastroenterologist, hematologist). The goal is to reduce serum ferritin level to 50–100 ug/L. Hemoglobin is also monitored and avoidance of iron and vitamin C supplements is recommended. There are no dietary restrictions recommended while an individual is undergoing therapeutic phlebotomy.
Treatment should be initiated when:
- Transferrin saturation (>45%) AND serum ferritin (>300 ug/L in men and post-menopausal women; >200 ug/L in pre-menopausal women) are elevated, particularly with the C282Y/C282Y and C282Y/H63D genotypes
A genetic predisposition to iron overload (e.g. C282Y/C282Y genotype) is not on its own an indication for treatment in the absence of abnormal iron indices. Serial assessment of serum ferritin and liver aminotransferase is recommended and treatment initiated when necessary.
WHEN SHOULD GENETIC TESTING FOR HEREDITARY HEMOCHROMATOSIS BE CONSIDERED?
Consider genetic testing for HFE-related hereditary hemochromatosis in adults with:
- Biochemical evidence of iron overload [>45% fasting transferrin saturation and elevated serum ferritin (>300 ug/L in men and post-menopausal women, >200 ug/L in pre-menopausal women)]
- Individuals with HFE-related HH occasionally demonstrate a normal transferrin saturation and an elevated ferritin. If clinical suspicion is high and/or the patient has a family history of HFE-HH, genetic testing is still warranted.
- Unexplained chronic liver disease and increased transferrin saturation.
- A first-degree relative (sibling, parent or child) where genetic testing identified C282Y homozygosity (genotype C282Y/C282Y)
- Symptoms of iron overload and a first-degree relative where genetic testing identified at least one copy of the C282Y pathogenic variant
- A family history confirmed or suggestive of hereditary hemochromatosis (see figure 1, higher suspicion when two or more are present in one individual)
Note: Many Canadian Genetics Clinics no longer accept referrals to arrange genetic testing for HFE-related HH. Connect with your local genetics specialist if you are unsure about how to arrange testing or if a referral may be indicated e.g. eConsult, phone the genetic counsellor on-call at your local centre.
Elevation of ferritin alone is not necessarily due to iron overload. Ferritin is an acute phase reactant and secondary causes of increased levels may be infection, chronic liver disease, iron-loading anemia, chronic inflammatory state, malignancy.
General population screening for HH is not recommended. Genetic testing in children is not recommended as HFE-related HH is an adult-onset condition. As HFE-HH is an autosomal recessive condition, the partner of an affected individual may consider genetic testing to better assess the risk to their children.
For guidelines on the management of patients with HH, see Kowdley et al. Am J Gastroenterol. 2019; PMID: 31335359.
Authors: S Morrison MS CGC, JC Carroll MD CCFP, GE Graham MD FRCPC and JE Allanson MD FRCPC
Updated: July 2023
Disclaimer:
· GECKO is an independent not-for-profit program that does not accept support from commercial or non-academic entities.
· GECKO aims to aid the practicing non-genetics clinician by providing informed resources regarding genetic/genomic conditions, services and technologies that have been developed in a rigorous and evidence-based manner with periodic updating. The content on the GECKO site is for educational purposes only. No resource should be used as a substitute for clinical judgement. GECKO assumes no responsibility or liability resulting from the use of information contained herein.
· All clinicians using this site are encouraged to consult local genetics clinics, medical geneticists, or specialists for clarification of questions that arise relating to specific patient problems.
· All patients should seek the advice of their own physician or other qualified clinician regarding any medical questions or conditions.
· External links are selected and reviewed at the time a page is published. However, GECKO is not responsible for the content of external websites. The inclusion of a link to an external website from GECKO should not be understood to be an endorsement of that website or the site’s owners (or their products/services).
· We strive to provide accurate, timely, unbiased, and up-to-date information on this site, and make every attempt to ensure the integrity of the site. However, it is possible that the information contained here may contain inaccuracies or errors for which neither GECKO nor its funding agencies assume responsibility.

