
Download the PDF here. View the point of care tool to assist in identifying patients most likely to benefit from referral to genetics. For a more comprehensive review, view the GECKO Messenger.
Bottom line: Epilepsy is a chronic brain disease that is characterized by an enduring predisposition to recurrent unprovoked epileptic seizures. A single gene mutation causes epilepsy in about 30% of affected individuals. Genetic testing should be considered for individuals with red flags, including: epilepsy with accompanying dysmorphic features, intellectual disability, autism and/or cognitive regression; drug-refractory epilepsy; epilepsy with multiple neurological co-morbidities; or a positive family history. Genetic testing may provide a specific diagnosis for the individual with epilepsy and may end the diagnostic odyssey. This may help to guide management, provide information on prognosis and more accurate recurrence risk counselling, and provide prenatal testing options. Importantly, a molecular diagnosis may bring closure for the family and help them to network with support groups.
Under review
What is epilepsy?
Epilepsy is a chronic brain disease characterized by an enduring predisposition to recurrent unprovoked epileptic seizures. Epilepsy is diagnosed when an individual has: 1) ≥ two unprovoked or reflex seizures (seizures consistently induced by a specific stimulus or trigger) more than 24 hours apart, 2) one unprovoked or reflex seizure and a high probability of having another seizure (e.g. a child with Sturge-Weber syndrome presenting with a first seizure) or 3) a recognizable epilepsy syndrome (e.g. an individual with a characteristic history and clinical presentation plus EEG findings consistent with a condition such as West syndrome).
How common is epilepsy?
Epilepsy is the second most common neurological condition.
What do I need to know about the genetics of epilepsy?
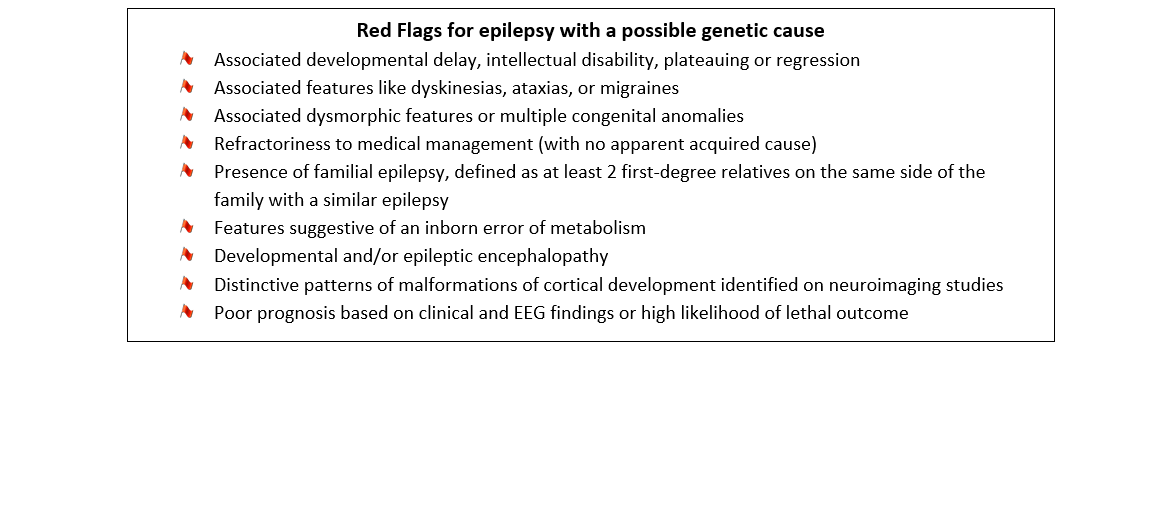
Epilepsy is best described as a group of conditions. Not all epilepsies are genetic in origin. Most commonly, a complex combination of genetic and non-genetic factors leads to a seizure disorder, with a genetic contribution estimated to be present in up to 70% of affected persons. For this reason, twins and first degree relatives of affected persons are at increased risk for epilepsy. Only a fraction of epilepsies as a whole can be explained by monogenic inheritance, with epilepsy due to a mutation in a single gene that can be detected by genetic testing occurring in about 30% of affected individuals. Certain types of epilepsy have a high likelihood of a genetic etiology. Refer to the ‘Red Flags for epilepsy with a possible genetic cause’ box below.
Current genetic testing methods have variable reported yields such as genomic microarray – 3 to 10%, targeted gene panels – 10 to 48.5%, whole exome sequencing – 11 to 72%. This variability in testing yields may be attributed to differences in the number of genes tested (in a targeted gene panel), research cohort size and inclusion criteria.
How is epilepsy usually evaluated?
Detailed clinical evaluation is the first step including evaluation of the epilepsy presentation (i.e. age of onset, seizure types, etc), developmental profile (any developmental delays or related issues), presence of additional neurological features (movement disorders, tone abnormalities, etc), and systemic involvement (heart or other organs). This assessment should also include documentation of any unusual facial features and/or skin findings, and relevant family history. Tests include electroencephalogram [EEG], brain MRI and metabolic screening depending on the epilepsy presentation. Investigations like video-EEG and brain MRI are usually indicated where the etiology is uncertain, the seizures focal or prolonged, or the affected individual is refractory to antiepileptic drugs.
How do i order genetic testing?
Many genetic tests for epilepsy are currently available, and the decision about which test to order involves a number of different factors ranging from clinical presentation to clinical utility. A detailed clinical evaluation is a mandatory pre-requisite, after which an epileptologist or geneticist will generally order genetic testing as indicated.
Individuals with the following types of epilepsy do not require genetic testing:
- Benign focal epilepsy
- Typical idiopathic generalized epilepsy (e.g. childhood absence epilepsy, juvenile myoclonic epilepsy)
- Isolated mesial temporal lobe epilepsy with hippocampal sclerosis
- A clearly acquired epilepsy (e.g. occurring secondary to head trauma, CNS infection, hypoxia)
- Simple febrile seizures (if presentation becomes complex or atypical, genetic evaluation may be warranted)
What do the genetic test results mean?
A positive result confirms a genetic cause, however, variable expressivity and incomplete penetrance must be kept in mind.
A negative result may not rule out the diagnosis of a genetic disorder. It means that the specific test did not pick up a particular genetic abnormality. Epilepsy syndromes show extensive genetic heterogeneity, and a negative test for a given gene/gene panel does not mean the person does not have the condition. Further epilepsy phenotyping and/or selection of a more appropriate genetic test or panel may be warranted.
Clinical utility and management
Identifying a genetic cause for the epilepsy may have significant clinical utility depending on the disorder identified. The diagnosis may have implications for treatment and further management, providing information about the natural history of the disorder, response to specific drugs, likelihood of associated neurological and other systemic co-morbidities, and prognosis, thus guiding follow up and surveillance. A diagnosis facilitates accurate risk recurrence counselling for future offspring and may direct the testing of “at-risk” family members.
Individuals with epilepsy contemplating pregnancy can be informed of the risks associated with certain anti-epileptic medication (e.g. valproic acid), the likelihood the medication will cause congenital anomalies or intellectual disability, and risks related to breastfeeding.
See www.geneticseducation.ca for the full GEC-KO Messenger on the genetics of epilepsy for more details. For general guidelines on epilepsy management, please refer to the Epilepsy Ontario provincial guidelines for management of epilepsy in adults and children V.1.2015.
Authors: P Jain MD, DM, D Dyment MD, FRCPC, O.C Snead III MD, FRCPC
Edited by the GECKO team: JE Allanson MD FRCPC FCCMG, S Yusuf MS CGC, JC Carroll MD CCFP
Disclaimer:
· GECKO is an independent not-for-profit program that does not accept support from commercial or non-academic entities.
· GECKO aims to aid the practicing non-genetics clinician by providing informed resources regarding genetic/genomic conditions, services and technologies that have been developed in a rigorous and evidence-based manner with periodic updating. The content on the GECKO site is for educational purposes only. No resource should be used as a substitute for clinical judgement. GECKO assumes no responsibility or liability resulting from the use of information contained herein.
· All clinicians using this site are encouraged to consult local genetics clinics, medical geneticists, or specialists for clarification of questions that arise relating to specific patient problems.
· All patients should seek the advice of their own physician or other qualified clinician regarding any medical questions or conditions.
· External links are selected and reviewed at the time a page is published. However, GECKO is not responsible for the content of external websites. The inclusion of a link to an external website from GECKO should not be understood to be an endorsement of that website or the site’s owners (or their products/services).
· We strive to provide accurate, timely, unbiased, and up-to-date information on this site, and make every attempt to ensure the integrity of the site. However, it is possible that the information contained here may contain inaccuracies or errors for which neither GECKO nor its funding agencies assume responsibility.

