Updated July 2024
|
|
- HTAD accounts for ~20-25% of all thoracic aortic aneurysms and dissections.
- Most individuals with HTAD do not have additional associated features (non-syndromic).
- HTAD presents at a younger age and is more aggressive than other TAA.
- Appropriate recognition of HTAD allows initiation of imaging surveillance in at-risk relatives.
- A positive genetic test result can help guide pharmacotherapy, determine vascular regions which require ongoing imaging surveillance, influence surgical threshold, and allow for cascade testing of at-risk relatives.
- In most families with HTAD, genetic testing does NOT identify the responsible genetic variant. Thus negative testing does not exclude HTAD and at-risk relatives would still need ongoing imaging surveillance.
- Pharmacological management for those with TAA may include:
- beta-blockers or angiotensin receptor blockers to limit aneurysmal dilation.
- avoidance of medications and recreational drugs with potential vasoactive effect (e.g. triptans, cocaine).
- Fluoroquinolones should be avoided as much as possible in anyone with aortic aneurysms or at risk for aortic aneurysm (thoracic or not, heritable or not), because of the associated increased risk of aortic dissectio
- Participation in competitive sports and isometric exercises are advised against.
|
More on HTAD can be found in the comprehensive GECKO deep dive and the concise GECKO on the run.
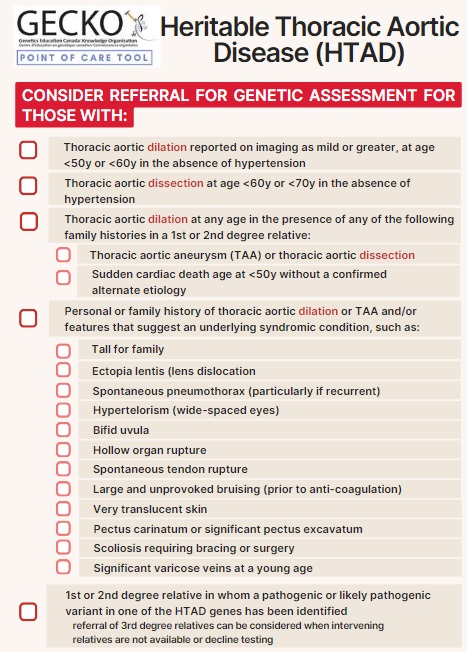
 Heritable Thoracic Aortic Disease (HTAD)
Heritable Thoracic Aortic Disease (HTAD)
