
Download the PDF here. View the point of care tool containing a road map of possible genetic tests and consultations for the individual with autism spectrum disorder. Access an education module with case-based learning here. For a more comprehensive review, view the GECKO Messenger.
Autism spectrum disorder (ASD) is a complex, genetically influenced disorder, affecting about 1 in 68 children. ASD is highly variable both in presentation and in etiology. In families where one child has ASD, the risk to subsequent siblings is about 10-19%. About 15-40% of individuals with ASD will have an identifiable contributing genetic cause. First tier genetic investigations for ASD are chromosomal microarray and fragile X syndrome testing. If an individual is determined to have ASD plus (signifying additional co-morbidities such as congenital anomalies, dysmorphic features, neurological symptoms e.g. seizures), additional investigations may be considered. A genetic diagnosis can potentially lead to guideline-based surveillance and management, tailored treatment options, opportunities to participate in clinical trials, information regarding natural history and prognosis, familial testing and more accurate recurrence risk counselling. Primary care providers who feel confident providing pre- and post –test counselling may be able to arrange first tier genetic investigations prior to or concurrent with referral for genetic consultation. Local laboratories may limit which providers can order these tests.
Updated Oct 2017
What is autism spectrum disorder?
Autism spectrum disorder (ASD) is a complex heterogeneous group of neurodevelopmental disorders affecting brain function and behaviour. The core features of ASD include pervasive impairments in communication and social interaction, repetitive behaviours and/or restricted interests1.
How common is ASD?
Recent surveillance data suggest that about 1 in 68 children is affected by ASD with males diagnosed about four times more often than females1,2.
How is ASD diagnosed?
Diagnosis of ASD is based on clinical criteria, the most recent of which are found in the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition [DSM-5]. A child may first be brought to attention following routine screening using a tool such as the validated Modified Checklist for Autism in Toddlers-Revised (M-CHAT-R™).
What causes autism spectrum disorder?
ASD is a genetically influenced disorder caused by genetic, epigenetic (factors that affect gene expression and activity) and non-genetic (environmental) factors1,3,4. For couples who have a child with ASD, the chance for each of their subsequent children to be diagnosed with ASD is about 10-19%3,5,6. Recurrence risks can sometimes be more accurately predicted if a genetic etiology is known.
About 15-40% of individuals with ASD will have an identifiable contributing genetic cause, depending on the study population and the type of genetic technology used3,7.
About 25% of individuals with ASD will have complex ASD or ASD plus, meaning that autistic features are accompanied by congenital anomalies, dysmorphic features and/or neurological findings (see Figure 1).
What are the Red Flags that suggest genetic consultation and/or genetic testing?
Once an ASD diagnosis is confirmed, a provider can consider the red flags below to determine if the individual has isolated ASD or ASD plus. A genetics referral could be made at that time. Alternatively, a provider who is comfortable providing pre-test counselling and post-test follow-up could begin the first tier genetic testing and refer upon receipt of results. Local laboratories may limit which providers can order these tests. Contact your local genetics centre for more.
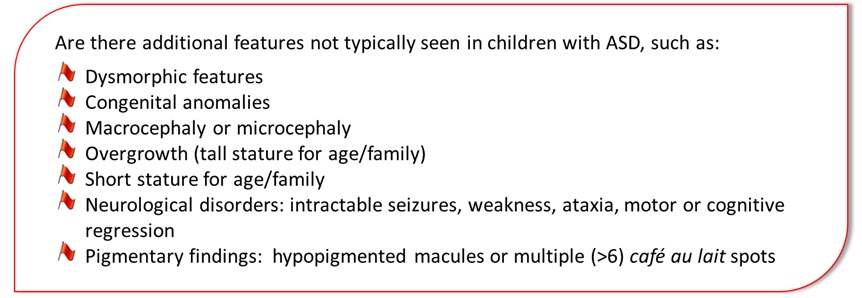
Figure 1. Red flags to alert a health care provider that their patient’s ASD is complex, also known as ASD plus, and could benefit from a genetic consultation.
What can my patient expect at a genetic consultation for autism spectrum disorder?
The role of a clinical geneticist is to identify the etiology of the ASD where possible, with the hope of improving management of the individual and providing genetic counselling for the family9. A clinical genetics consultation includes a review of the patient’s prenatal, perinatal, medical and family histories, and a physical examination to document growth parameters (such as head circumference) and look for evidence of dysmorphic features1.
The Canadian College of Medical Geneticists (CCMG) recommends that chromosomal microarray and fragile X syndrome testing be the first tier laboratory investigation for any male or female whose ASD and/or other developmental disability is unexplained after a thorough history and physical examination10. Second tier investigations may be guided by presentation. Clinical geneticists may ofter genetic testing for a single gene syndrome (e.g. Rett syndrome, Cowden syndrome) or a next-generation sequencing panel which could include tens to thousands of genes.
What are the benefits of genetic consultation [with or without genetic testing]?
Advances in genomic technology have provided the opportunity for many families to receive an answer to the question ‘why does my child have ASD’. A genetic diagnosis can potentially lead to guideline-based surveillance and management, tailored treatment options, opportunities to participate in clinical trials, information regarding natural history and prognosis, familial testing and more accurate recurrence risk counselling. In the absence of an identifiable genetic etiology, a recurrence risk (RR) range can be quoted based on empirical studies. For families where one child has ASD, the RR is about 10-19%5,6. Males are at higher risk than females. Couples with two children with ASD have a higher RR, around 30%3. The more distant an affected relative is, the lower the RR.
What are the limitations and complexities of genetic testing for autism spectrum disorder?
There are several complexities to genetic testing such as uncertain results. Not every genomic variation has been classified as either benign or pathogenic. This sort of result can neither confirm nor rule out a specific genetic etiology and can be frustrating for families and providers. Another complex result is an ASD ‘risk variant’ with incomplete penetrance. This is one of the most difficult scenarios for genetic counseling3. In this circumstance it is difficult to determine the chance of familial recurrence. This genetic change may have been inherited from an affected, mildly affected or even unaffected parent.
Not all individuals will have an identifiable genetic diagnosis. While the genetic contribution to ASD has been well established, today’s technology and knowledge will identify a genetic etiology in about 15-40% of individuals with ASD. Individuals and families who attend a genetic consultation with the expectation of receiving a diagnosis may feel disappointed.
Find the contact information for your local genetics centre here.
For community support and research opportunities for your patient and his/her family, see Autism Speaks Canada.
For a complete Reference and Resource list please see the GEC-KO Messenger.
A point of care tool can be found here.
For an excellent review on ASD diagnosis in the primary care setting, please see Anagnoustou and colleagues1.
Authors: S Morrison MS CGC, JC Carroll MD CCFP, MT Carter MD FRCPC FCCMG, and JE Allanson MD FRCPC FCCMG
Disclaimer:
· GECKO is an independent not-for-profit program that does not accept support from commercial or non-academic entities.
· GECKO aims to aid the practicing non-genetics clinician by providing informed resources regarding genetic/genomic conditions, services and technologies that have been developed in a rigorous and evidence-based manner with periodic updating. The content on the GECKO site is for educational purposes only. No resource should be used as a substitute for clinical judgement. GECKO assumes no responsibility or liability resulting from the use of information contained herein.
· All clinicians using this site are encouraged to consult local genetics clinics, medical geneticists, or specialists for clarification of questions that arise relating to specific patient problems.
· All patients should seek the advice of their own physician or other qualified clinician regarding any medical questions or conditions.
· External links are selected and reviewed at the time a page is published. However, GECKO is not responsible for the content of external websites. The inclusion of a link to an external website from GECKO should not be understood to be an endorsement of that website or the site’s owners (or their products/services).
· We strive to provide accurate, timely, unbiased, and up-to-date information on this site, and make every attempt to ensure the integrity of the site. However, it is possible that the information contained here may contain inaccuracies or errors for which neither GECKO nor its funding agencies assume responsibility.

